

Being A diabetic patient doesn’t mean that you forbid from any carbs, sweet’s….ex)But it means that you should control about your eating and life style .
What is diabetes?
high blood glucose concentrations (hyperglycemia) resulting from Defects in insulin secretion, insulin action, or both
Categories of diabetes:
Categories of Glucose Intolerance:
- Prediabetes
- Type‐1 Diabetes Miletus
- Type‐2 Diabetes Miletus
- Gestational Diabetes Miletus
Other categories: diabetes associated with specific genetic syndromes (such as neonatal diabetes and, genetic defects in insulin action, diseases of the exocrine pancreas (such as cystic fibrosis), endocrinopathies, (such as acromegaly or Cushing’s syndrome), drug or chemical induced ( treatment of HIV/AIDS or after organ transplantation), infections, and other illnesses.
Medical nutritional therapy:
Optimal control of diabetes requires the restoration of normal carbohydrate, protein, and fat metabolism.
Reduce calorie intake can lead to reductions in A1C of 0.3% to 2.0% in adults with T2DM and improvements in medication doses and quality of life.
weight loss interventions implemented in people with prediabetes and newly diagnosed with T2DM have been shown to be effective in improving glycemic control>weight.
loss diets are not sustainable.
Optimal control of diabetes requires the restoration of normal carbohydrate, protein, and fat metabolism.
• Through the collaborative development of individualized nutrition interventions and ongoing support of behavior changes, health care professionals can facilitate the achievement of health goals for the person with diabetes.
Eating pattern:
For only controlling blood glucose Patient should limit carbohydrates containing food Which is in many types of food like :
- Dairy products (milk,yogurt)
- Starchy products(white rice,bread,noodles..ex)
- Fruits
- Starchy vegetables (potatoes,corn,pees)
Carbohydrate intake:
- Starches are rapidly metabolized into 100% glucose during digestion, in contrast to sucrose, which is metabolized into only approximately 50% glucose and approximately 50% fructose.
- Fructose has a lower glycemic response, which has been attributed to its slow rate of absorption and its storage in the liver as glycogen.
- Care should be taken to avoid excess energy intake and to avoid displacing nutrient dense food choices.
• People with or at risk for diabetes avoid sugar‐sweetened beverages (soft drinks, fruit drinks, energy and vitamin‐type water drinks containing sucrose, high fructose corn syrup, and/or fruit juice concentrates) to reduce the risk of worsening the cardio-metabolic risk profile and to prevent weight gain.
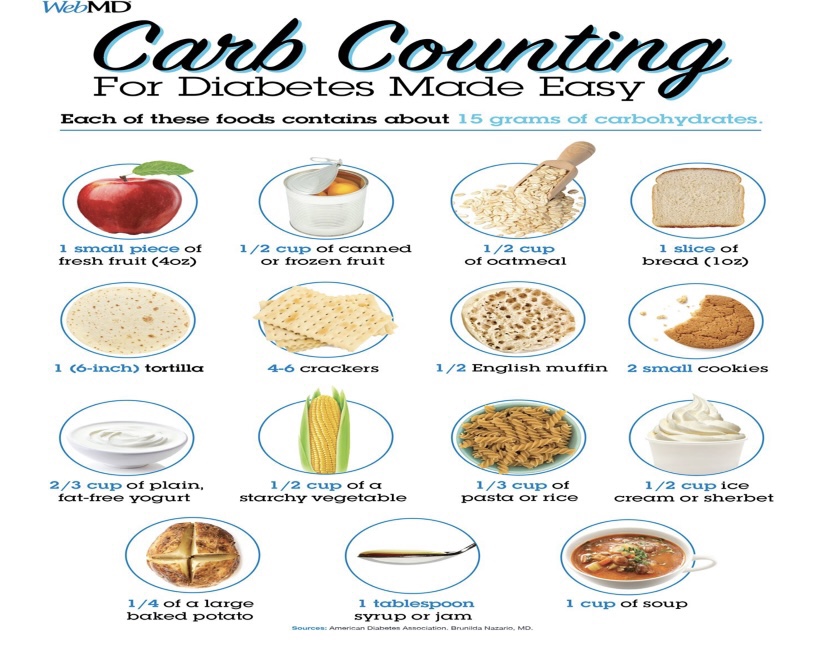
Carbohydrates counting:
An eating plan method based on the principle that all types of carbohydrate (except fiber) are digested, and that the majority of carbohydrates are absorbed into the bloodstream as molecules of glucose.Carbohydrate foods include starches, such as breads, cereals, pasta, rice, beans and lentils, starchy vegetables, crackers, and snack chips; fruits and fruit juices; milk, milk substitutes, and yogurt; and sweets and desserts.One carbohydrate exchange (or serving) is a portion of food containing 15 grams of carbohydrate.
Micronutrients and herbal supplements:
Use of routine vitamin or mineral supplementation is not recommended in people with diabetes who do not have underlying deficiencies .Certain supplements may be helpful in lowering blood sugar levels :cinnamon, chromium, alpha‐lipoic acid (ALA), and berberine.
- Cinnamon
Doses of 120 mg/day to 6 g/day for 4 to 18 weeks reduced levels of FPG,total cholesterol (–15.60 mg/dL), LDL cholesterol (–9.42 mg/dL), and triglycerides (–29.59 mg/dL) while increasing levels of HDL cholesterol (1.66 mg/dL).
Caution: when combining cinnamon (in pill form) with other blood glucose lowering herbs and supplements, as taking cinnamon with some antidiabetic drugs may cause hypoglycemic effects.
- Berberine
An alkaloid found in a variety of medicinal plants (tree turmeric) Berberine significantly lowered FBG, A1C, triglyceride, and insulin levels in patients with T2DM similar to those of metformin and rosiglitazone.
• Liver function was improved greatly in these patients by showing reduction of liver enzymes treatment with berberine or metformin(0.5 g three times per day).
• After the 3 months, the hypoglycemic effect of berberine can be similar to that of metformin.
• Significant decreases in A1C ,FBG ,postprandial blood glucose (19.8 mmol/L to 11.1 mmol/L), and triglycerides.
Physical activity in diabetes:
Exercise guidelines:
The variability of glucose responses to exercise contributes to the difficulty in giving precise guidelines for exercising safely.
➢Frequent blood glucose monitoring before, during, and after exercise helps individuals identify their response to physical activities.
➢To meet their individual needs, it is important to modify general guidelines to reduce insulin doses before (or after) exercise.
Exercise recommendations:
Adults with diabetes should be advised to perform at least 150 min/week of moderate intensity aerobic physical activity spread over at least 3 days/week with no more than 2 consecutive days with physical activity.
•In the absence of contraindications, adults with T2DM should be encouraged to perform resistance exercise at least twice per week with each session consisting of at least one set of five or more different resistance exercises involving large muscle groups.
• There is an additive benefit of combined aerobic and resistance training in adults with T2DM.
• Children with diabetes or prediabetes should be encouraged to engage in at least 60 min/day of physical activity with vigorous muscle‐strengthening and bone‐strengthening activities at least 3 days/week
• High‐risk patients should be encouraged to start with short periods of low‐intensity exercise and increase the intensity and duration slowly.
