
Nowadays there’s many people suffering from anemia due to many things, if the patient doesn’t care it could affects his quality of life .
Definition:
Anemia is present when there is reduction in number of RBCs & Hb content of blood with decreased O2 carrying capacity of blood in relation to age & sex. Other factors including pregnancy and altitudes also affect hemoglobin levels and must be taken into account when considering whether an individual is anemic.
Classification:
Etiological:
•Deficiency anaemia e.g. Iron↓ – Vit B 12 ↓ –
Folic acid ↓
• Aplasticanaemia
• Haemolyticanaemia.
• Haemorrhagicanaemia.
Morphological:(according to blood indices)
• Microcytic hypo chromic:
Iron deficiency
Thalassaemia
Sideroblastic anaemia
• Normocytic normochromic: Acute blood loss.
• Macrocytic normochromic:
Megaloblastic anaemia (folic acid or vitamin B-12 deficiency ).
Iron deficiency Anaemia:
Iron deficiency is the most common
micronutrient deficiency worldwide.
• Iron deficiency is the result of long term negative iron balance. Iron stores are progressively diminished and no longer meet the needs of normal iron turnover.
Iron metabolism :
Source:
(absorbed better than non Heam iron, about 15%
absorbable)
Non Heam iron : legumes & Vegetables. (A bout 3% – 8% absorbable)
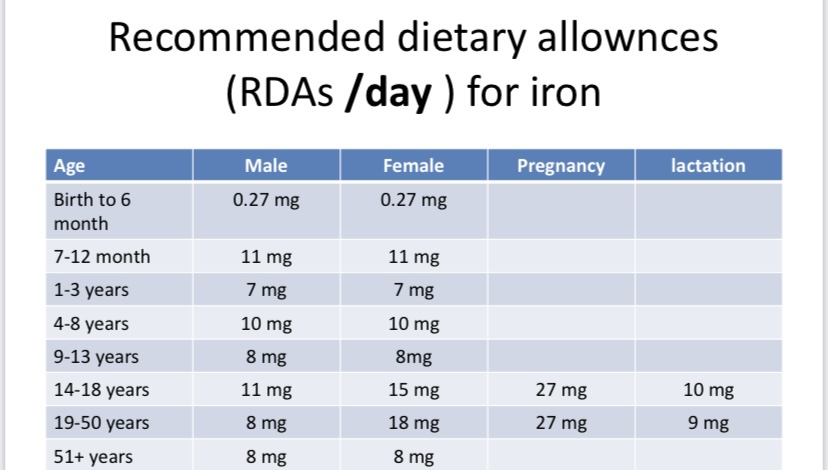
Requirements:10 mg/day of which1 mg is absorbed.
Absorption: ↑with vit C, ↓with phosphates, phytates , oxalic acids, excess ca and tannins
•Amount of iron absorption depend on:
iron status (absorption is more in iron deficient persons and during pregnancy and after blood loss).
•Normal GIT function (HCL ↑ absorption) Type of iron in diet (Heam & non Heam) Dietary factors that ↑ or ↓ iron absorption.
Causes of iron deficiency Anemia:
- Inadequate intake:
• Infancy after 6m ( the American Academy of pediatrics recommended all exclusively breastfed infants should receive iron drops of 1 mg/kg/day at 4 months of age [22] to augment the low levels of iron in mother’s milk ).
• anorexia.
• Old age. - Absorption:
• Mal_absorbtion (post-gastrectomy & chron’s disease), phytates(cereals), drugs (antacids) - Increase Demand:
• pregnancy, growing Child, erythropoietin therapy. - Chronic blood loss:
• (haemorrhage, especially GIT bleeding, Ankylostoma, Vaginal bleeding.
Diagnosis of iron deficiency Anemia:
Fatigue, Headache, Faintness and Breathlessness
• Pallor, angular stomatitis, red glazed shiny tenedr tongue
• Palpitation, Tachycardia
• Heart failure
• Brittle nails, loss of luster and Koilonychia (spooning)
• c/p of the cause: ankylostoma, GIT or Vaginal bleeding
To diagnose iron deficiency anemia:
•Serum iron : low 60 to 170 micrograms per deciliter (mcg/dL), or 10.74 to
30.43 micromoles per liter (micromol/L)
• (TIBC ) A total iron-binding capacity test measures the blood’s ability to attach itself to iron and transport it around the body : increased 240 mcg/dL to 450 mcg/dL
• Transferrin saturation*: low (s.iron/TIBC×100)(N: 25-50%)
• Serum Ferritin : low For men, 24 to 336 micrograms per liter. For women, 11 to 307 micrograms per liter (a low serum ferritin level reflects depleted iron stores)
• RDW (red cell distribution width) measures the differences in the volume and size of your red blood cells (erythrocytes) : increase (N R 12.2 to 16.1 percent in adult females and 11.8 to 14.5 percent in adult males ).
Management of Anaemia:
•Prevention of IDA
• Treatment of the underlying cause
• Iron therapy (supplement)
1)Oral iron (3-6 mg/kg/day)of elemental on empty stomach, if possible e.g: feroglobin cap
2)Parental iron
• Dietary management.
• General recommendations
1)Prevention of IDA:
•Full term infant are born with sufficient iron stores to prevent iron deficiency anemia for the first 4-5 months of life.
• Baby should be breast fed colostrums and mature milk, both have 49% absorbable iron this is sufficient with available fetal stores till baby doubles the birth weight.
•Weaning foods :from 6 months onwards should have one iron rich dietary item and iron supplementation be given as recommended as nutritional iron deficiency is most common between 6-24 month of life.
• Pregnant women: provide iron supplements during the last 2 trimester as daily iron requirements increase.
2)Treatment of the underlying cause:
Iron therapy (supplement)
•Oral iron (3-6 mg/kg/day)of elemental, if possible e.g: feroglobin cap, ferrosanol cap
The patient should be told that the stool will become dark with oral iron therapy.
Iron is best absorbed when taken on an empty stomach, with water or fruit juice (adults: full glass or 8 ounces; children: 1⁄2 glass or 4 ounces), about 1 hour before or 2 hours after meals. However, to lessen the possibility of stomach upset, iron may be taken with food or immediately after meals.
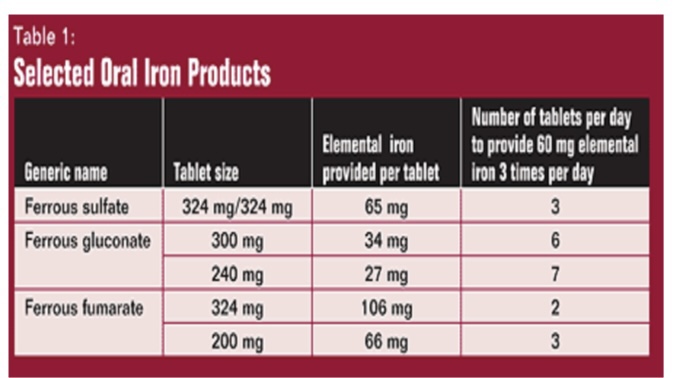
This is by ferrous sulfate 300 mg tab. (60 mg elemental iron/tab)
Dose:
1 tab. T. d. s. (give about 200 mg elemental iron/D)
It is best absorbed if given before meals but it is very irritant so it is given after meals vitaminC to increase its absorption.
In case of iron intolerance give ferrous sulfate twice or shift to ferrous gluconate, if no response consider parental nutrition.
Duration of therapy:
•For 4 – 10 weeks till Hb becomes normal
•Then smaller doses for about 3-6 months to replenish iron stores.
Failure of oral iron:
• Wrong diagnosis.
• Failure to take tablets..
• Malabsorption.
• Chronic hemorrhage.
• Chronic infection.
Dietary management:
Dietary sources of iron:
•Liver, red meat > poultry & fish
•Plants are generally not good sources because of oxalate, phytate, tannins e.g green leafy vegetables, legumes, whole grains, dried fruits, molasses.
General recommendation:
•Combine heme and non heme iron foods together at the same meal to increase absorption of iron from non heme food.
• Include vitamin c rich food together with iron rich foods (include in meal fruits juices as orange juice or another source of ascorbic acids as cabbage, carrots or cauliflower).
• Include meat fish poultry at meals. •Soak beans for several hours in cold water before you cook them.
• Decrease coffee and tea consumption and separate its drinking from 1-2 hours later.
• Cooking non heme food in iron pots.
• Change meal pattern (consume milk cheese and other dairy.
product as snacks between meals rather than at meal time.
•Consume foods containing inhibitors at meals lowest in iron content, e.g a breakfast of a low iron cereal (bread or corn) consumed with tea or milk products; this meal pattern can provide adequate calcium without hampering iron nutrition.
Reference:
https://www.webmd.com/search/search_results/default.aspx?query=anemia
https://scholar.google.com/scholar?q=anemia+nutrition+&hl=en&as_sdt=0,5
